
Been writing on Rural and Inside-city hospitals and the shortage of funding for them, the shopping for up of the identical by bigger entities, and the abuse of the 340B program by the bigger hospital. As soon as the bigger hospital buys the inner-city hospital, there’s a tendency to chop providers and in addition abuse the 340B program. Rural hospitals are much less funded than their metropolis cousins. Packages akin to Medicaid and Medicare pay lower than their smaller margins than what could also be acceptable attributable to bigger margins at their metropolis cousins. This additionally performs out in staffing as there is probably not sufficient work to keep up the staffing for specialised providers.
Not a lot modified for the Covid funding as higher quantities of funding per mattress went to the lager hospitals. Initially, smaller hospitals had been underfunded because the funding was directed elsewhere. It was not until the top, did smaller entities obtained funding.
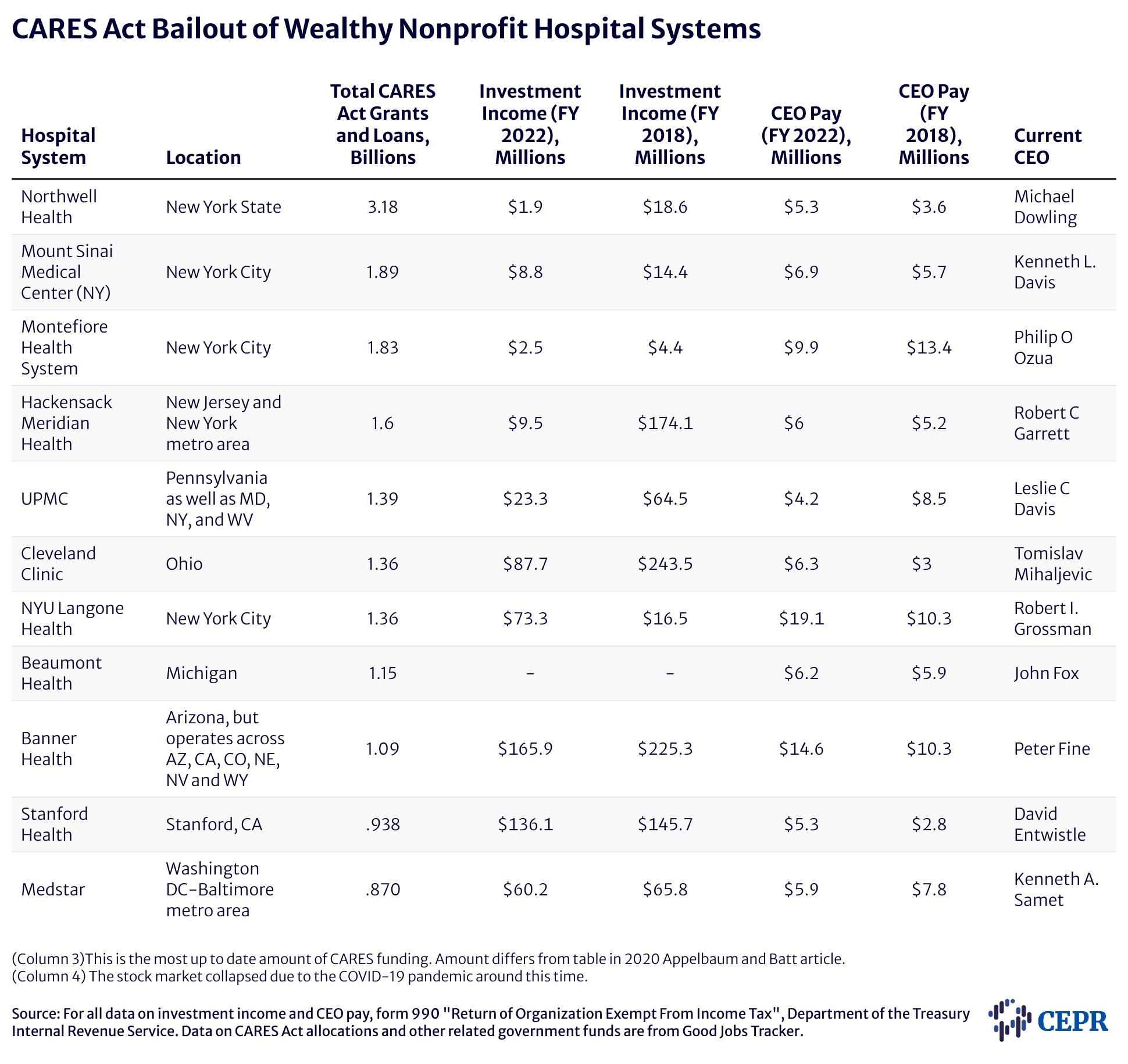
CARES Act Funding: Lethal Inequities in Hospital Bailouts, CEPR
In the course of the first and largest part of COVID-19 stimulus funding, $50 billion {dollars} of reduction was allotted to hospitals and different supplier organizations by a basic distribution of funds by the Well being Assets and Providers Administration (HRSA). HRSA allotted $30 billion based mostly on the organizations or clinician’s share of complete Medicare fee-for-service reimbursements in 2019 (Ellison 2020). The remaining $20 billion was allotted to hospitals based mostly on the hospital’s internet affected person income in 2019 (Liss 2020).
The final distribution was not based mostly on a hospital’s want for assets to deal with the pandemic and hospitals and different recipients weren’t required to make use of these funds for treating sufferers. Based mostly on these formulation the place sufferers had been extra more likely to be coated by Medicare or personal insurance coverage, the wealthier hospitals obtained extra funding. Extra funding than security internet hospitals and neighborhood well being facilities, the place sufferers are extra seemingly on Medicaid or uninsured (Abramson 2020).
Personal insurers usually pay almost double what Medicare pays for all hospital providers (Lopez, Neuman, Jacobson, and Levitt 2020). Notably, the system didn’t take note of whether or not the hospital handled giant numbers of COVID-19 sufferers and didn’t require hospitals to make use of CARES Act funds for his or her care. The primary part of funding got here with no strings connected.
Excessive reimbursement can come from having extra privately insured sufferers coming by the door or with the ability to cost larger charges to non-public insurance coverage firms due to their market energy. If a hospital dominated the market on the level of the HHS funding, they had been more likely to do effectively with the system. A Kaiser Household Basis examine discovered hospitals with the bottom share of income from personal insurance coverage obtained half as a lot per hospital mattress as their counterparts. These counterparts with the best share throughout the first $50 billion basic distribution wave of CARES Act funding in April 2020 (Schwartz and Damico 2020).
Additionally the wealthier hospitals with larger ranges of Medicare reimbursements, larger personal pay sufferers, or larger prior internet revenues obtained emergency funding from the Supplier Reduction Fund (PRF) and excess of did hospitals with higher want. Extra funding than these hospitals these counting on Medicaid or serving rural or lower-income communities.
Based mostly on share of personal insurance coverage income, the highest 10 p.c of hospitals obtained $44,321 per hospital mattress. They had been extra more likely to be for-profit establishments, had bigger working margins. These hospitals had been additionally much less more likely to be instructing hospitals and offering much less uncompensated care (a.okay.a. charity care) (Schwartz and Damico 2020). The 2 largest hospital chains, HCA Healthcare Inc. and Tenet Healthcare Corp., each of which personal tons of of hospitals, obtained $5.3 billion and $2 billion in loans and grants, respectively, within the first wave (Terhune 2020). Inside months, HCA returned to robust monetary well being with shares hovering and 38 p.c larger earnings than the earlier yr (Abelson 2020). The chain finally returned a big portion of its reduction (Pifer 2020). Together with Kaiser Permanente, it was one of many few rich hospital techniques to take action.
Hospitals and neighborhood well being facilities serving poorer populations and receiving most of their income from Medicaid, versus Medicare and personal insurers, went with out or obtained little or no of the preliminary $50 billion CARES Act funding pot. On common, they obtained simply $20,710 per hospital mattress.
Solely $2.6 billion of the $50 billion paid out went to Medicaid and CHIP suppliers. Many of those establishments had been both in rural areas or poor city communities the place COVID-19 an infection charges had been larger than within the geographies served by rich hospitals (Schwartz and Damico 2020). The disparity in income sources of those two teams of hospitals over many a long time has led to monetary instability of the hospitals serving most of America’s poorest communities. These are the hospitals inundated with COVID-19 sufferers within the early days of the pandemic. Moreover, these are the hospitals that, within the fast aftermath of the pandemic, obtained the least CARES Act funding to satisfy the problem.
Educational Medical Facilities usually have entry to a security internet of economic assets security internet hospitals don’t. Rich donors, endowments, and funding earnings enabled these and different well-endowed hospital techniques to construct substantial reserves. Regardless of this disparity in monetary assets, CARES Act funding nonetheless favored hospitals that would extra simply maintain the financial blow of the pandemic (see Desk 1). Analysis reveals the hospitals with vital money readily available obtained extra CARES Act PRF funding per mattress than did hospitals with negligible money obtainable. Whereas hospitals with at the very least 76 days of money readily available obtained $88,000 per mattress, hospitals with lower than per week of money readily available obtained $22,000 per mattress on common (Grogan et al. 2021).
Pushback from public well being specialists and others led to reforms in how later rounds of PRF funds had been distributed. The focused allocations that handed in Might 2020 made funds obtainable to hospitals that had been most impacted by COVID-19, together with smaller and financially strapped neighborhood hospitals in addition to giant educational medical facilities with excessive COVID-19 caseloads. These are the reduction targets and quantities:
– $20.7 billion “high-impact” fund meant for hospitals hardest hit by COVID-19,
– $10.9 billion to rural suppliers,
– $13.1 billion to security internet hospitals,
– $4.8 billion to expert nursing services,
– $4.7 billion to nursing dwelling an infection management, high quality, and efficiency,
– and at last $1.6 billion for youngsters’s hospitals and tribal well being suppliers (Coughlin 2022).
For the focused funding based mostly on COVID-19 prevalence; academic-affiliated hospitals with larger belongings previous to COVID-19 and hospitals having larger numbers of COVID-19 circumstances obtained larger ranges of funding. But once more, the smaller important entry hospitals obtained decrease ranges of economic help per mattress than their wealthier counterparts (Cantor et al. 2021).
Many hospitals which had been primarily rural hospitals and people serving poor communities, had been missed within the first three basic distribution phases of CARES Act distributions and high-impact distributions. This inequity was addressed to a higher extent within the fourth and remaining distribution of PRF funds which allotted a further $8.2 billion to those hospitals within the new Biden administration’s American Rescue Plan (ARP).
This was lower than a yr after the beginning of the pandemic and was an enchancment from early rounds of stimulus. Nonetheless, the disparity in almost all of the rounds of CARES Act funding got here on the heels of years of unequal funding of U.S. hospitals.
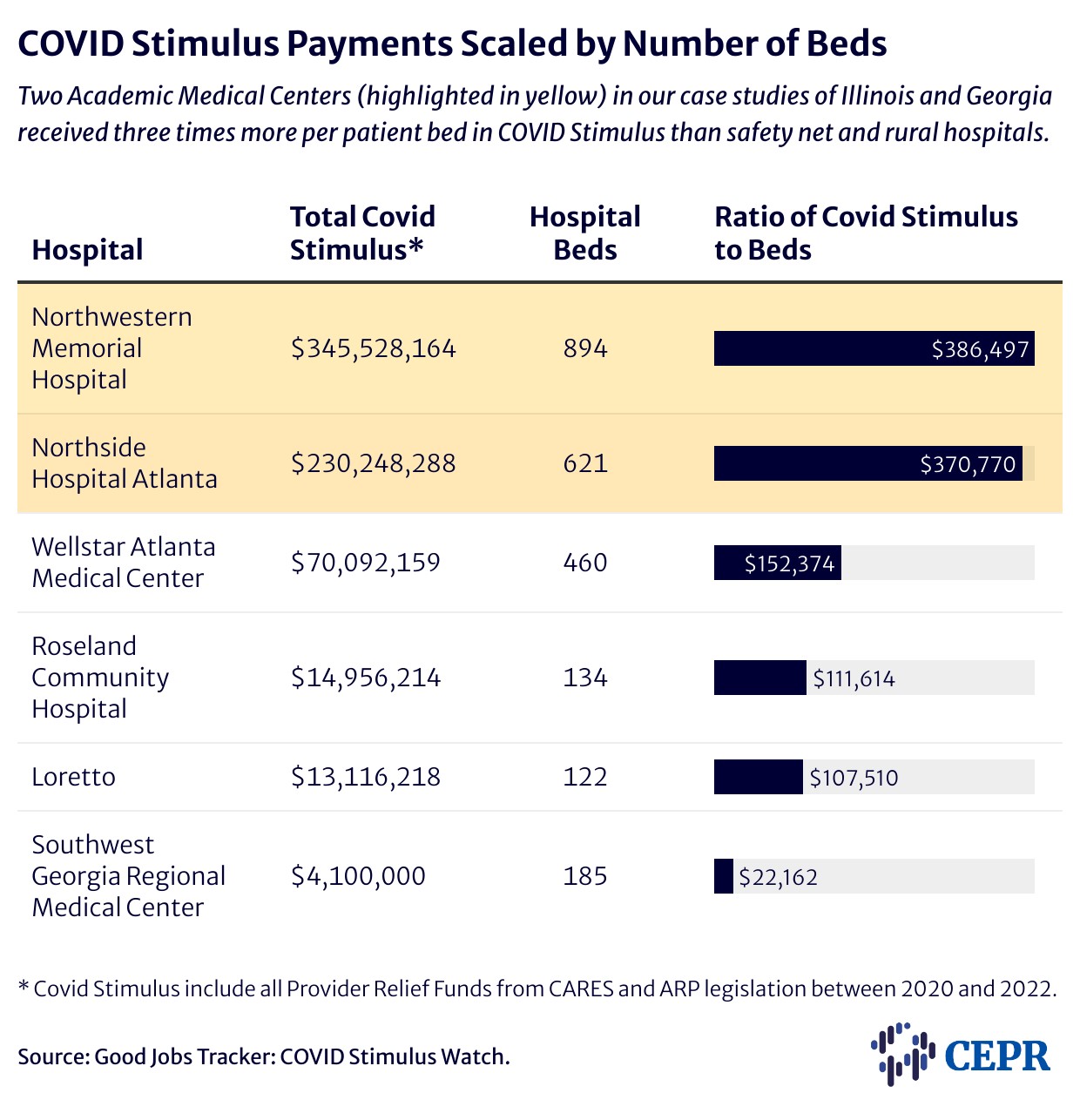
Desk 2 shows the COVID Stimulus offered to hospitals in our case research under in relation to the variety of hospital beds at every.
Illustrated within the CEPR report are the results of inequities in funding on well being outcomes of COVID-19 sufferers by analyzing the allocation of CARES Act funds to 2 states: Georgia and Illinois, and the life and dying results for sufferers. Each of those research will be discovered right here:
6.2.1 Georgia: A complete of $3.2 billion in CARES Act reduction was allotted to Georgia as of early December 2020. Round 40 p.c went to only 20 suppliers, leaving the greater than 10,000 suppliers and services within the state to share the rest (Shakoor, Gee, Rapfogel 2020). and right here . . .
6.2.2 Illinois: Chicago’s two-tier well being system illustrates the stark distinction between the allocation of CARES Act funds to security internet hospitals and to hospitals in college techniques. Take a look at Chicago’s Northwestern Memorial funding per mattress versus Chicago’s Loretto and Roseland Neighborhood hospital funding per mattress.
The supply of well being care assets a facility needed to deal with COVID-19 sufferers performed a significant position in sufferers’ well being outcomes and whether or not they survived the virus. Counties with decrease staffing ranges had been related to larger COVID-19-related deaths (Epané 2023) as had been hospitals whose bodily plant included fewer intensive care unit beds (Janke et al. 2021). It mattered the place you lived and which hospital you had entry to. Counties with larger per-capita incomes tended to have higher resourced well being care services and thus decrease COVID-19-related deaths (Epané 2023). Black, Latino, and Native American individuals died at a lot larger charges than white individuals (Hill and Artiga 2022). Residents of rural communities additionally suffered larger charges of COVID-19-related deaths than did city residents. Initially, city counties had larger charges of COVID-19-related deaths, particularly on the pandemic’s begin. Nonetheless, current evaluation reveals that over the long run, sufferers from rural counties skilled larger mortality charges and tended to be readmitted extra often following COVID-19 hospitalization (Yousufuddin 2024).
