
That is the boring stuff on healthcare. The best way to think about the prices of a rural emergency division care in a small rural hospital when it’s not in fixed use. And what occurs when the inhabitants is small and the prices equal the funds taken in by its operation. The article supplies a superb basis portraying these prices.
by Heart for Healthcare High quality and Fee Reform
The one most important service that rural hospitals present is a 24/7 Emergency Division. Though emergency departments at small rural hospitals do not need the potential to deal with extreme trauma circumstances and emergencies requiring highly-specialized companies, neither do many city hospital EDs. The first roles all EDs carry out are to rapidly and precisely diagnose well being issues, present any obligatory remedy to the sufferers, and switch the small set of sufferers who want specialised care to a trauma middle, stroke middle, and so forth. Residents of rural communities who do not need entry to an Emergency Division could also be extra prone to die or expertise problems that would have been prevented.
This part will study the prices concerned in working Emergency Departments at small, rural hospitals. The main target on this part can be on the essential ED go to itself, not on any further companies a affected person could obtain throughout the go to which are delivered by different hospital departments, corresponding to a laboratory take a look at or an imaging examine. The prices of delivering these different companies can be examined individually beneath.
The Variety of ED Visits at Small Rural Hospitals
It’s cheap to anticipate that the price of an Emergency Division will depend upon what number of visits the ED has. Rural hospitals which have a small variety of inpatient admissions appear much less small when one counts ED visits. Nearly all of small rural hospitals had fewer than 5,000 ED visits in 2017, i.e., about one go to each 2 hours.1 Nevertheless, there may be additionally appreciable variation within the quantity of ED visits amongst these hospitals; 10% of small rural hospitals (i.e., hospitals with lower than $30 million per 12 months in whole bills) had greater than 11,000 ED visits in 2017, whereas one other 10% had fewer than 1,000 visits.
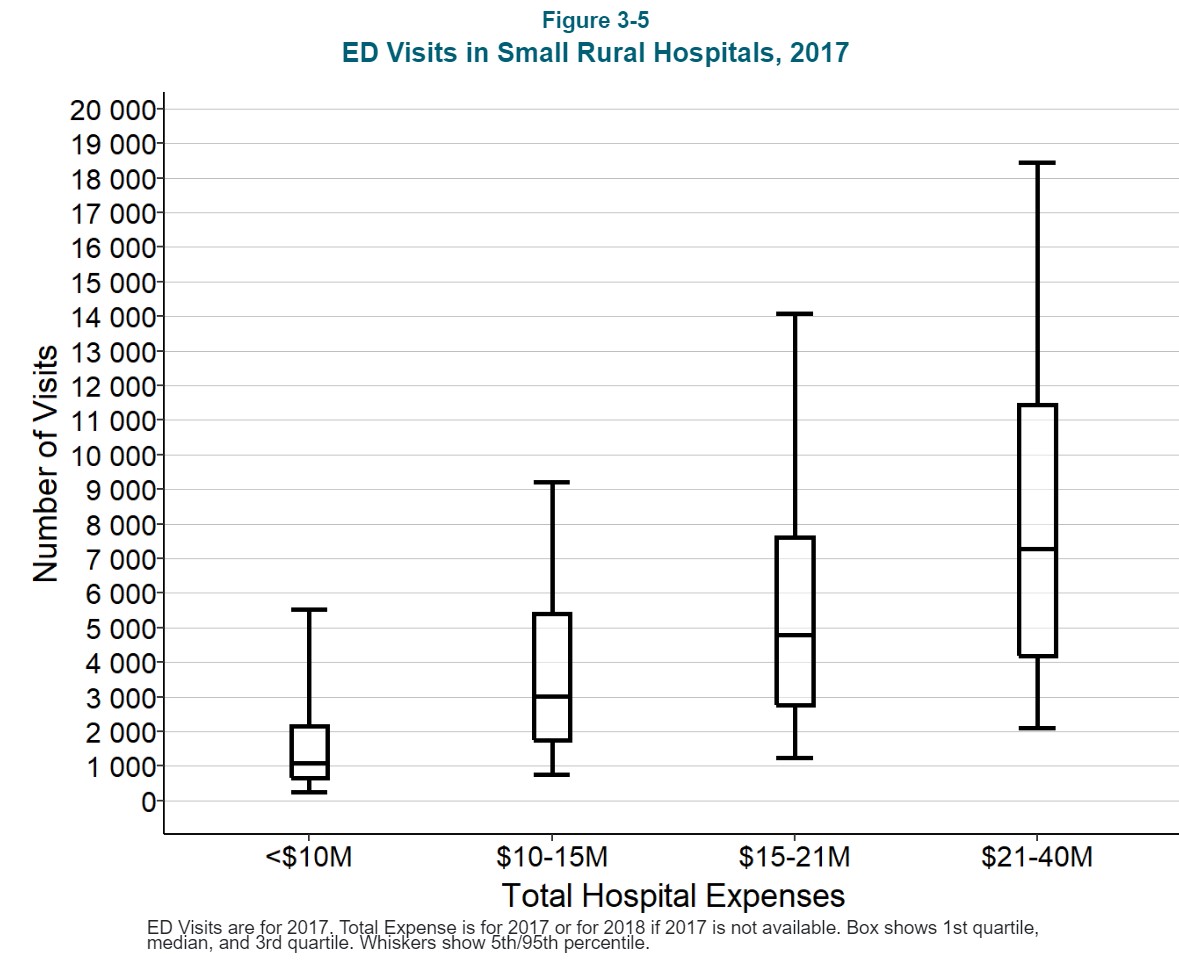
The big variation within the variety of visits is because of a wide range of components, together with the dimensions of the group the hospital serves, the age and well being standing of the residents locally, the variety of companies and staff locally, the variety of vacationers who go to the group, and the group’s proximity to an interstate freeway. Importantly, the variety of ED visits may also depend upon the supply of main care locally. For instance, a hospital with no Rural Well being Clinic will probably have extra ED visits than a hospital that has an RHC as a result of, with out quick access to a main care observe, extra residents of the group might want to use the ED for non-emergency care.
The Price of Working an ED With 10,000 Visits Per Yr
Every hospital’s price report consists of info on the full price of working its emergency division, however it’s unattainable to find out why some EDs are costlier than others, even with the identical variety of visits, as a result of there may be little or no info on the person parts of that price. Particularly, personnel prices could be anticipated to be the only largest part of the price of an ED, however there isn’t a info out there on the variety of physicians, nurses, or different workers who work within the ED, the variety of hours they work, or the wage charges they’re paid.2
Nevertheless, for the reason that ED must ship high-quality care to sufferers who include a variety of issues at unpredictable instances, one can estimate the extent of staffing {that a} hospital would probably want with the intention to present that care and the way the staffing would change based mostly on the quantity of ED visits the ED receives.
Doctor Staffing
An Emergency Division that has 10,000 visits per 12 months will see a mean of 1 new affected person each hour. Though not each affected person who involves the ED might want to see a doctor, the ED might want to have a doctor out there in case they do, so there must be at the least one doctor on obligation always.3
The quantity of visits will usually be larger at sure instances of the day, days of the week, and months of the 12 months. For instance, hospitals in communities with numerous seasonal companies, corresponding to these in agriculture and tourism, could have larger volumes of ED visits throughout some months than others. Nevertheless, since productiveness requirements for Emergency Departments usually assume that an ED doctor can handle 2-3 visits per hour, it’s going to usually not be obligatory for an ED with 10,000 visits per 12 months to have any multiple doctor on obligation at a time besides throughout distinctive circumstances.4
Nevertheless, for the reason that ED is a 24/7 operation, the hospital must make use of or contract with at the least 4 full-time equal (FTE) physicians with the intention to have one doctor within the ED always.5 (The precise variety of physicians will depend upon the variety of shifts every doctor is prepared and capable of work every week, the period of time the physicians have to spend in persevering with schooling, trip days, and so forth. Some rural hospitals have to rent or contract with a number of physicians, every of whom come to the group for a brief time frame, with the intention to have one “full-time equivalent physician.)” 6
A hypothetical hospital that employs 4 FTE physicians to workers its ED might want to spend about $1.2 million to take action if it pays the physicians a wage of $120/hour with advantages equal to twenty% of the wage. Nevertheless, the precise price of using emergency physicians can differ considerably from group to group and from 12 months to 12 months relying on a hospital’s means to draw and retain physicians.
If a doctor retires or resigns, a hospital will usually want to rent a brief doctor to fill in whereas a everlasting alternative is discovered, and the hourly price of the short-term doctor will usually be considerably larger than the price of a everlasting worker. Many rural hospitals contract with nationwide ED staffing firms with the intention to eradicate the burden of sustaining a full staffing complement and to make the price of staffing the ED extra predictable7, however this will improve the general price of the ED as a result of the staffing firm must be paid greater than the physicians themselves obtain.
Nursing Employees
Along with a doctor, the ED may also want at the least one Registered Nurse (RN) across the clock to assist in triaging, treating, and discharging sufferers. Since a nurse will usually have to spend extra time with every affected person than the doctor does, it’s doable that one nurse can be inadequate if a number of sufferers come to the ED on the identical time or if the sufferers have extra critical situations. Small rural hospitals will sometimes take care of a number of visits or extra critical circumstances by having a nurse from the inpatient unit come to the ED to supply help. (The necessity for this backup protection will have an effect on the nurse staffing ranges the hospital will want within the inpatient unit, as mentioned in a later part.) If the upper volumes happen at predictable instances, the hospital could have to have two nurses on these shifts.
As a way to have at the least one nurse within the ED always, a hospital must make use of as many as 5 FTE RNs.8 If the hypothetical hospital pays RNs $38/hour and supplies advantages equal to twenty% of wage, the full price for the 12 months can be greater than $400,000. Right here once more, although, the price of using nursing workers will differ throughout communities and over time based mostly on the power of particular person hospitals to draw and retain nurses and the way a lot it prices them to fill vacancies quickly whereas everlasting replacements are being recruited.
Different Employees
The hospital will probably additionally want at the least one non-clinical workers member to examine sufferers in, assist members of the family, and so forth. in order that the doctor and nurses can concentrate on offering scientific companies to the sufferers. As a way to have such a workers member within the ED always, the hospital might want to make use of 4-5 FTEs. Assuming a $16/hour wage and 20% advantages, this may price the hypothetical hospital an extra $170,000 per 12 months.
Different Direct Prices
Nearly the entire direct prices of working an Emergency Division are related to the physicians, nurses, and different workers. The prices of any drugs used and different provides which are billed to a affected person individually are ordinarily assigned to a separate hospital price middle (these prices can be mentioned individually in a later part), so non-personnel direct prices for the ED itself will usually be comparatively small.
Oblique Prices
Lastly, the operation of the ED additionally will depend on the hospital offering house and utilities, upkeep for tools, housekeeping, billing for affected person visits, payroll and advantages for workers, medical information, and so forth. Consequently, a portion of the hospital’s prices for these actions have to be allotted to the ED to correctly signify the full price of working the ED. Usually, these oblique prices improve the full price of an ED by about 50% past the personnel and different direct prices mentioned above.9
Complete Price
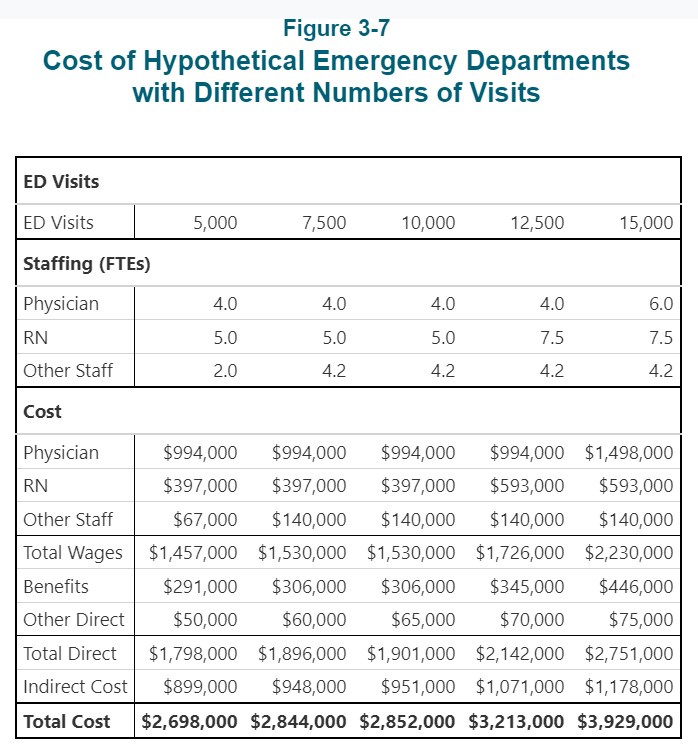
These 5 parts collectively suggest that it’s going to probably price the hypothetical hospital practically $3 million to ship companies to 10,000 ED sufferers throughout the 12 months.

The Price of Working an ED with Extra or Fewer Visits Per Yr
How does the associated fee differ for an ED with extra or fewer visits?
- For a hospital ED with 7,500 visits per 12 months (i.e., 25% fewer than the ten,000 visits mentioned above), there’ll nonetheless be virtually one go to each hour, so this ED may also want one doctor, one nurse, and a 3rd workers member on obligation around the clock. Different direct prices can be barely decrease with fewer sufferers and the oblique prices assigned to the ED may be decrease. Utilizing the identical assumptions about wage and profit charges as for the hypothetical hospital mentioned above, the full price of the ED can be 96%-97% of the price of the ten,000 go to ED, although there are 25% fewer visits.
- Even when a hospital ED has solely 5,000 visits per 12 months, it’s going to usually have to have a doctor and nurse on obligation across the clock, since it could have multiple go to each two hours on common. It’s doable that the ED would possibly have the ability to keep away from utilizing a 3rd, non-clinical workers member throughout sure instances of the day or week when the quantity of visits is low, notably if there may be somebody working in a distinct division on the hospital who can carry out the identical capabilities when wanted, however this might solely scale back the personnel prices by a comparatively small quantity. The whole price of an ED this dimension would probably nonetheless be greater than 90% as a lot as the price of the 7,500-visit ED, although there are 33% fewer visits.
- If the ED has 12,500 visits per 12 months (25% greater than the ten,000 visits on the hypothetical hospital mentioned earlier), it’s going to have a mean of 1.5 visits per hour, which may additionally usually be managed with a single doctor on obligation. Nevertheless, due to the larger potential for delays throughout peak instances, a hospital could select to have an extra nurse on some shifts, which can improve the full variety of nurses wanted to workers the ED general. In consequence, direct prices and oblique prices could also be 13% larger than on the ED with 10,000 visits.
- If the ED has 15,000 visits per 12 months (50% greater than the ten,000 go to ED), it’s going to have a mean of practically 2 visits each hour. As a result of ED visits don’t happen at a relentless price all through the day and week, it’s probably that the ED could have greater than 3 visits per hour throughout its busiest instances, which is greater than a single doctor can safely deal with. Consequently, the hospital will probably want to rent further physicians with the intention to have two physicians on obligation throughout the high-volume shifts, along with a bigger variety of nurses. This might improve the price of working the ED by 45% over the associated fee on the 10,000 go to degree, though this improve continues to be smaller than the 50% improve in visits.
The Price of Working an ED with Even Fewer Visits
Most small rural hospitals have fewer than 5,000 ED visits per 12 months. If the variety of visits is lower than about 10 per day (i.e., lower than one go to each 2-3 hours), the hospital might be able to workers the ED in another way, at the least throughout some shifts. Nevertheless, its means to take action will depend upon what different companies the hospital gives, the supply of different physicians locally and their willingness to assist workers the ED, and the supply of distant assist companies from bigger hospitals:
- If the hospital operates a Rural Well being Clinic in or subsequent to the ability the place the ED is positioned, the physicians, nurse practitioners, or doctor assistants who work within the clinic might depart the clinic and go to the ED to see a affected person who involves the ED throughout regular clinic hours.10
- At a hospital with a Rural Well being Clinic(RHC), the RHC physicians/clinicians might additionally present on-call protection throughout night time or weekend shifts when go to volumes are decrease. If there are different main care physicians locally, they might even be prepared to supply on-call protection for the ED.
- A really low-volume ED might doubtlessly use emergency-trained nurses to workers the ED if the hospital can organize for telemedicine assist from emergency physicians at a bigger hospital.11
- If the nursing workers within the hospital’s inpatient unit is massive sufficient (e.g., as a result of the hospital has numerous swing-bed sufferers), if the inpatient unit is shut sufficient to the ED, and if the quantity of ED visits is low sufficient, the hospital might depend on the inpatient unit nurses to workers the ED when a affected person arrives, both throughout some shifts or all shifts, fairly than having a nurse assigned completely to the ED.
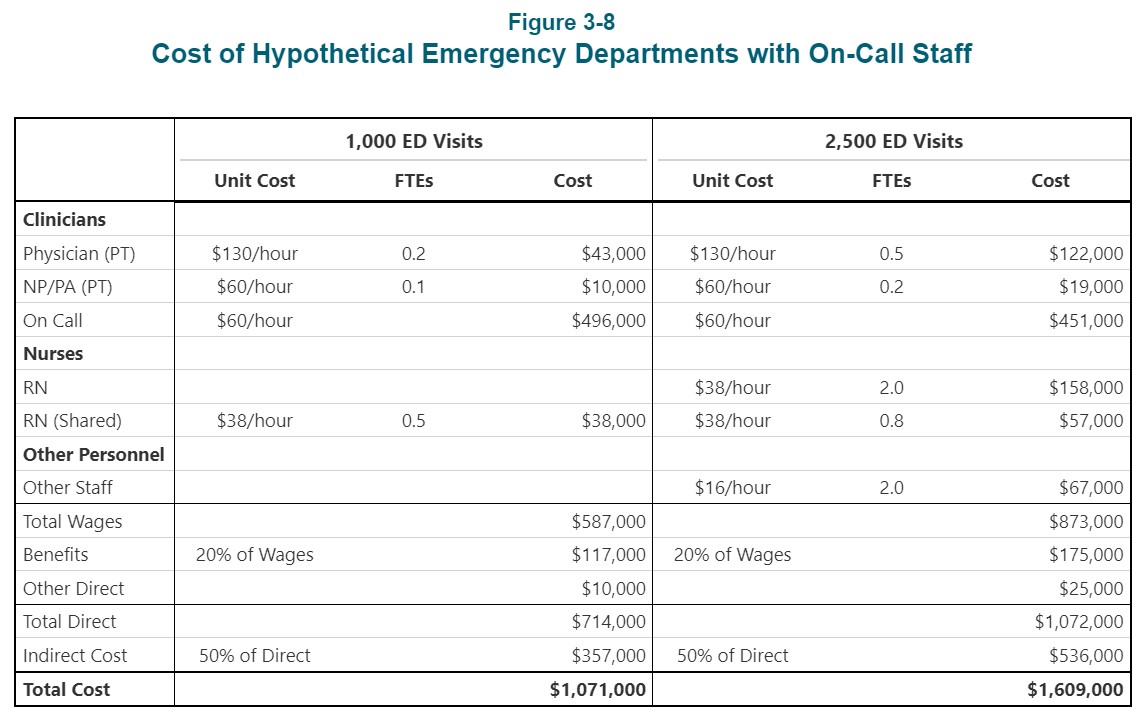
The desk beneath exhibits what the associated fee could be to function a hypothetical ED that has 1,000 visits per 12 months. This represents a mean of fewer than 3 visits per day or lower than one go to each 8 hours. The hospital the place this ED is positioned is assumed to additionally function a Rural Well being Clinic staffed by each a doctor and a Nurse Practitioner (NP). The doctor and the NP take accountability for seeing sufferers who come to the ED throughout clinic hours.
As well as, the Rural Well being Clinic clinicians and a number of different physicians locally are assumed to be prepared to contract with the hospital to supply on-call assist, i.e.. They might agree to come back to the ED rapidly if and when a affected person arrives. The instance additionally assumes that there could be no devoted nurses within the ED, and that one of many nurses from the hospital’s inpatient unit would go to the ED when a affected person arrives. The whole price of this association is simply over $1 million. That is nonetheless about 40% of the price of the ED with 10,000 visits, although there are solely one-tenth as many visits.
A hospital with 2,500 visits per 12 months (about 6 visits per day) would possibly nonetheless have the ability to depend on physicians on the Rural Well being Clinic and locally to diagnose and deal with sufferers. Nevertheless, it could be extra problematic to rely solely on nurses from the inpatient unit to workers the ED, notably throughout busier instances, so it’d have to make use of further nurses for this objective. As proven within the desk, the full price could be about $1.6 million.
Subsequent up? Complete Service Line Prices and is fee satisfactory to cowl smaller and rural hospitals?
